Everyone’s experience of remote learning is different. His may have been a lot less negative than many others (even though it was obviously negative) All that closing the schools would achieve is deferring the “chaos” anyway. Omicron is going nowhere (until the next variant arrives) and is benign to the point of irrelevance in this age group.
There comes a point where life has to normalise as much as possible and I think we’ve reached that point. My kids school is similarly strained. Absent teachers and pupils galore. But whatever short term impact this has on learning (and let’s not pretend that remote learning isn’t an absolute disaster for many kids) is outweighed by the benefits of socialising with their friends every day and getting back into a familiar routine. Even a return to school sports (a rarely mentioned casualty of closing them down) has been hugely beneficial for mental (and physical) health.
We got a lot of feedback from students that our (in-person) labs were the high points of their (otherwise virtual) semesters. The one I taught was strictly distanced and much quieter than it used to be pre-covid, but they still liked it. So even with much older students, even with restrictions, in-person is important. I get that.
But I'm teaching in a rich private university that could afford to reduce class sizes, install HEPA filters, give every student a fresh surgical mask* for every lab, this was before even delta... It was a microbio course with most of the students aiming for medicine or research, they were old, informed, and motivated enough to respect masking and distancing rules. Our group of 18 had either zero or one case over 4 months of teaching. I am asthmatic, fat and unfit but not obese, live alone, and am 30, not zero risk but not terrible.
In the US, where this debate is very much part of the culture war:
Many regular schools have crowded classes, no ventilation, often no testing, young kids with very different information and motivations and hence very variable masking, older and at-risk teachers with multiple comorbidities, all living with others in their household. Basic safety requirements demanded by teachers unions are not being provided by city govts even when they are funded.
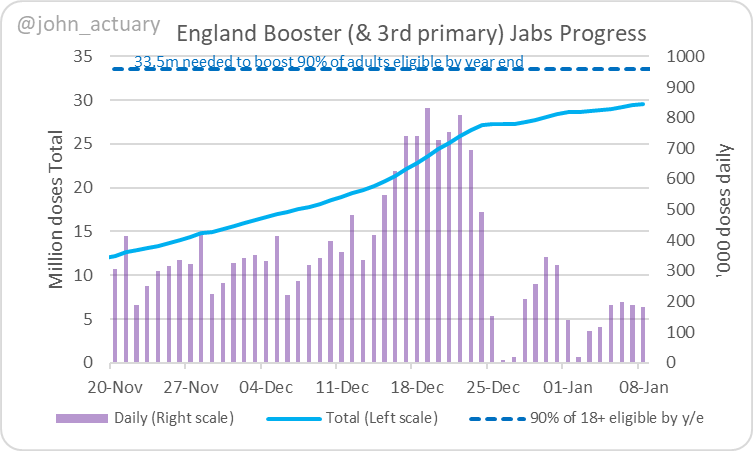
Inevitably, as you said, it's spreading like wildfire through schools (an amazing graph
here). And while most people aren't getting anything serious, with hospitalisations and deaths rising
as quickly as in previous waves, those who do get serious symptoms might well have to fend for themselves.
Add to this that the people pushing fairy-tale science in 2020 regarding schools are back and prominently pushing re-opening, it's bound to increase suspicion. (For example, Emily Oster, an economist who in 2020 said covid can't spread much in schools and created a
deliberately undercounted dashboard, whose data she used in the WaPo and NYT, is back prominently on CNN with the same recommendations)
And that's the impact on teachers and households without going into the students themselves. Since your post I've seen these stories:
Persons
aged <18 years with COVID-19 were more likely to receive a new diabetes diagnosis >30 days after infection than were those without COVID-19 and those with prepandemic acute respiratory infections. Non–SARS-CoV-2 respiratory infection was not associated with an increased risk for diabetes.
https://www.cdc.gov/mmwr/volumes/71/wr/mm7102e2.htm?s_cid=mm7102e2_w
“Long COVID”, where symptoms of COVID-19 persist for months after an initial infection, could be emerging as a chronic disease in Finland, Minister of Family Affairs and Social Services Krista Kiuru said on Friday.
Speaking at a news conference, she referred to a Finnish expert panel’s summary of more than 4,000 international studies which showed
one in two adults and around 2% of children may experience prolonged symptoms connected to COVID-19.
“Around 20% see long-term cognitive impairment,” Roine added, warning that the incidence of neurological diseases such as Alzheimer’s or Parkinson’s could increase sharply following a COVID-19 infection.
https://www.reuters.com/article/us-...THGOz12jqsVoUZ7ArIyDJX42a6F43SPSZ15bVKtFyW9bQ
It's better to say
1. We have lost the current phase of the fight to contain covid
2. Full re-opening of schools means an estimated x deaths and possibly y long-term issues for students and teachers (it's tough to model households)
3. But we must prioritise face-to-face human social contact over other issues.
And let parents and teachers decide accordingly. Clarity instead of what seems to be haphazard, dysfunctional nonsense.
 Don’t feel personally attacked, I haven’t even read your posts. It was in response to what I’ve seen on Twitter countless times and I’m sure in this thread too. I glanced over recent posts and saw models/predictions being discussed.
Don’t feel personally attacked, I haven’t even read your posts. It was in response to what I’ve seen on Twitter countless times and I’m sure in this thread too. I glanced over recent posts and saw models/predictions being discussed.")