A number of droplet generation measurements have found that the majority of exhaled droplets during breathing are in the sub-micron range, while coughing and sneezing can produce large droplets. Wells [14] first defined large droplets as those over 100um in aerodynamic diameter. The mechanism of droplet formation and origin is also associated with virus and bacteria load in droplets, as pathogens are usually limited to certain areas of the body. Lindsley et al. used the quantitative polymerase chain reaction (qPCR) to measure the influenza virus in aerosol particles from human coughs. Some 35% of the detected influenza RNA was contained in particles>4um in diameter, 23% in particles of 1-4um, and 42% in particles<1um, showing not only that coughing by patients emits aerosols containing the influenza virus, but also that much of the viral RNA is contained within particles in the respirable size range.
...droplet size seems the most important factor affecting dispersion and deposition [deposition refers to a droplet impacting on a surface]
...The number of droplets during a single cough can be as high as 3000
...Xie et al. extended the study by analysing the cough jet as a steady round jet, and found that the expired droplets can travel up to 1.5-2 m. The effect of turbulence was not considered. Most computer modelling studies also have not properly considered the impact of turbulence. Klettner et al. theoretically demonstrated that the effect of turbulence significantly increases the transmission distance and spread of droplets in a hospital room.
[Note that a round jet is simply a flow of air which is ejected from a pipe which has a circular diameter. "Steady" means that they looked at an air flow whose average velocity (in time) at some location, normally the centre of the pipe, was constant. Turbulence refers to a state of fluid motion which is, generally, chaotic-like. Think of "fast" moving flows..]
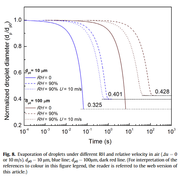
...The evaporation process of a single droplet was first studied, as shown in Fig. 8. It takes 0.066 s and 6.63 s for droplets with initial sizes of 10um and 100um, respectively, to become droplet nuclei in still and dry conditions (RH=0, and the relativevelocityDu=0 m/s). The evaporation time here seems proportional to the square of the initial droplet diameter d^2....Similar results have been presented in other studies [RH is the relative humidity].
... The ambient humidity has a significant effect on the evaporation rate of droplets, as the evaporation time increases to 1.52 s (23-fold) and 199.0 s (30-fold), respectively, in humid conditions (RH=90%).Due to the Kelvin effect, small droplets have a smaller final normalised diameter (0.401) compared with large droplets (0.428), as shown in Fig. 8.